By Miranda Milana, Psy.D.
Pediatric Neuropsychologist
When families seek a neuropsychological evaluation for their child, it’s usually because they’re looking for a deeper, more comprehensive understanding of their child’s profile—including both strengths and challenges. This kind of evaluation helps answer important questions about how a child learns, thinks, manages emotions, and interacts with others.
By gaining this insight, we can better support a child in all areas of life—at school, at home, with friends, and in community settings. Sometimes, however, the most valuable piece of the puzzle doesn’t come from test scores at all.
In some cases, your neuropsychologist may determine that observing your child in their natural learning environment—a school observation—can provide crucial information that simply can’t be gathered in an office setting.
What Is a School Observation?
A school observation involves a trained professional—usually the neuropsychologist conducting your child’s evaluation—visiting your child’s school to observe them in real time.
This observation might include time spent watching your child:
- During classroom instruction
- In social settings like lunch or recess
- While transitioning between classes
- In additional services, such as speech/language therapy or occupational therapy
The purpose is to see how your child functions across different settings and situations throughout their school day.
Why Is a School Observation So Valuable?
You might wonder: if the evaluator already has detailed testing results, rating forms from parents and teachers, and information from the intake appointment and outside providers, why observe at school?
Even the best testing environment can’t fully replicate real-world situations. In a quiet, 1:1 testing setting, a child might appear regulated, focused, and engaged—but in a classroom filled with distractions and increased demands, their behavior and overall presentation might look very different. A school observation helps us understand how a child manages in the real-world environments where challenges often arise.
Observations allow us to:
- Identify situations that may be triggering challenging behaviors (like transitions, group work, or unstructured time)
- Determine whether a child is well-matched with their peers or may be in the wrong instructional group
- Notice social dynamics—Are they connecting with peers? Are they withdrawn or overly controlling during play?
Another critical area we assess during school observations is whether the learning environment is a good fit for your child:
- Is the classroom appropriately structured?
- Are staff using the tools and supports outlined in the IEP?
- Does your child respond well to the strategies, like visual schedules or token boards, being used?
Observing how a child responds to the classroom setup and supports can help determine whether their current environment is truly meeting their needs—or if changes are required to allow them to access the curriculum.
When Is a School Observation Recommended?
Not every evaluation requires a school observation, but there are several situations where it can provide especially meaningful insight. Examples include:
- A child who struggles with behaviors at school that aren’t seen at home or during testing
- A child who performs well on standardized tests but is reported to be having a hard time keeping up in class
- Uncertainty about whether the child’s current classroom or program is the right fit for their learning profile
- Questions about whether the child would benefit from a different instructional approach, such as a language-based classroom or one using ABA methods
At NESCA, our clinicians are trained to determine when a school observation would add helpful information to the evaluation process. We view it as one of many tools to build the most accurate picture of your child’s needs.
What to Expect During the Observation
If you and your evaluator decide that a school observation would be helpful, we’ll coordinate the visit with your child’s school—with full permission from you and the school team.
On the day of the observation:
- The evaluator typically sits in the back of the classroom, making every effort not to disrupt the flow of the day.
- The goal is to blend in and observe naturally occurring interactions and behaviors.
- Observations are done in a respectful, non-intrusive manner with the sole purpose of helping your child.
Afterward, the evaluator will include a summary of the observation in the written report, and the insights gained will be integrated into the diagnostic impressions and recommendations.
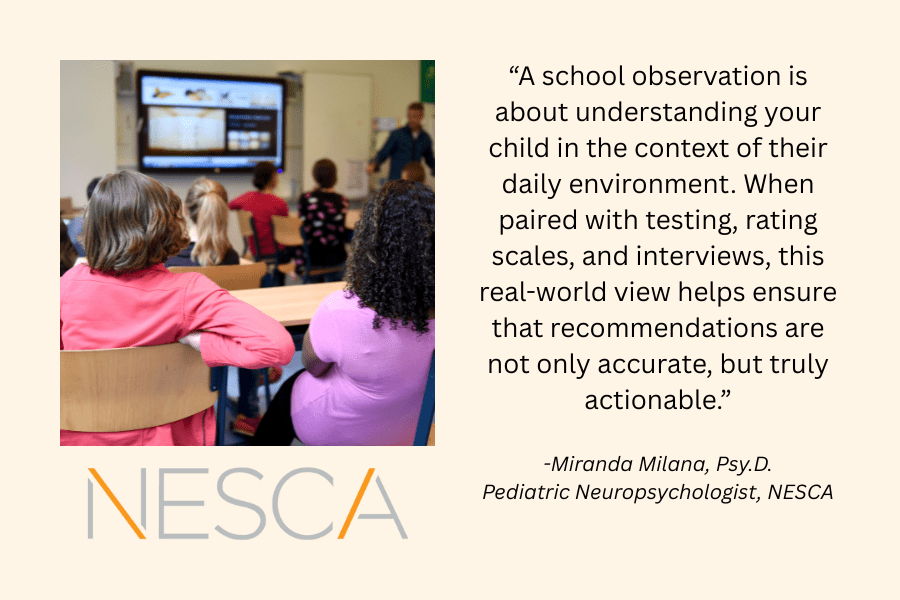
A school observation is about understanding your child in the context of their daily environment. When paired with testing, rating scales, and interviews, this real-world view helps ensure that recommendations are not only accurate, but truly actionable.
If you have any questions about the school observation process—or want to know whether it might be helpful for your child—don’t hesitate to reach out to your evaluator. We’re always here to help guide you through the process and help your child get the support they need to succeed.
About the Author
Dr. Miranda Milana provides comprehensive evaluation services for children and adolescents with a wide range of concerns, including attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).
attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).
Dr. Milana places great emphasis on adapting her approach to a child’s developmental level and providing a testing environment that is approachable and comfortable for them. She also values collaboration with families and outside providers to facilitate supports and services that are tailored to a child’s specific needs.
Before joining NESCA, Dr. Milana completed a two-year postdoctoral fellowship at Boston Children’s Hospital in the Developmental Medicine department, where she received extensive training in the administration of psychological and neuropsychological testing. She has also received assessment training from Beacon Assessment Center and The Brenner Center. Dr. Milana graduated with her B.A. from the University of New England and went on to receive her doctorate from William James College (WJC). She was a part of the Children and Families of Adversity and Resilience (CFAR) program while at WJC. Her doctoral training also included therapeutic services across a variety of settings, including an elementary school, the Family Health Center of Worcester and at Roger Williams University.
Dr. Milana grew up in Maine and enjoys trips back home to see her family throughout the year. She currently resides in Wrentham, Massachusetts, with her husband and two golden retrievers. She also enjoys spending time with family and friends, reading, and cheering on the Patriots, Bruins, Red Sox, and Celtics.
To book an appointment with Dr. Miranda Milana or another expert NESCA neuropsychologist, please complete our Intake Form today.
NESCA is a multidisciplinary pediatric neuropsychology practice with offices in Newton, Plainville, and Hingham, Massachusetts; Londonderry, New Hampshire; and the greater Burlington, Vermont region, serving clients from infancy through young adulthood and their families. For more information, please email info@nesca-newton.com or call 617-658-9800.


 attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).
attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).


 attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).
attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).

 attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).
attention deficit disorders, communication disorders, intellectual disabilities, and learning disabilities. She particularly enjoys working with children and their families who have concerns regarding an autism spectrum disorder. Dr. Milana has received specialized training on the administration of the Autism Diagnostic Observation Schedule (ADOS).
Connect with Us